Hospital Bill (Sample)
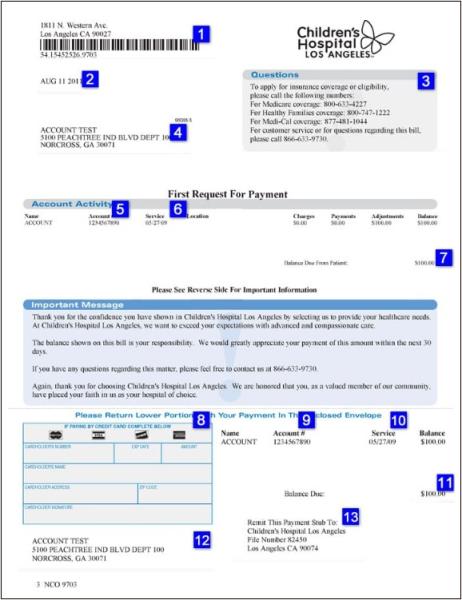
- Hospital Payment Information
Send your payment(s) to this Children's Hospital Los Angeles address. - Statement Date
This date indicates the day that your invoice was prepared and mailed to you. - Billing Customer Service Numbers
This area has the numbers to call if you have any questions about your bill. - Your Contact Information
The name and mailing address represents the information we have on file for the person(s) responsible for payment of the invoice. If you have moved or need to have this information sent to the appropriate party, contact us at 1-866-633-9730. - Account Number
This is your account number. - Service Date
This date represents the date of your child's hospital visit and services referenced on your bill. - Amount Due
This is the balance and the amount that you owe. - Credit Card Billing Information
Fill out this area of the form in detail if you are planning to pay by credit card. Be sure to include your signature and signature code (the 3- or 4-digit code on the back of your credit card). Note: Children's Hospital Los Angeles accepts MasterCard, Discover, Visa and American Express. - Account Number
This is your account number. - Service Date
This date represents the date of your child's hospital visit and services referenced on your bill. - Amount Due
This is the balance and the amount that you owe. - Your Contact Information
The name and mailing address represents the information we have on file for the person(s) responsible for payment of the invoice. If you have moved or need to have this information sent to the appropriate party, contact us at 1-866-633-9730. - Hospital Payment Information
Send your payment(s) to this Children's Hospital Los Angeles address.